How Estrogen Dominance Affects MCAS and Histamine Intolerance and How to Test Hormones
Estrogen and histamine are interconnected. And both trigger mast cells, which can lead to flares in Mast Cell Activation Syndrome (MCAS) symptoms.
You may have noticed that your mast cell symptoms get worse at certain times of your menstrual cycle. Or maybe they ramped up as you started going through perimenopause or menopause.
It’s no coincidence!
In this post we’ll share more about the connection between hormones, mast cells, and mediators (like histamine).
You’ll learn about:
- What estrogen dominance is
- The roles of progesterone and estrogen
- How estrogen, Histamine Intolerance, and Mast Cell Activation Syndrome connect
- How you can test hormones properly
- Why testing is so important
Very simply put, estrogen dominance is an imbalance of hormones that leads to more estrogen than progesterone. You’ll read more about this in just a bit.
And for so many of the women we work with, estrogen dominance has been a mast cell trigger.
Hormone imbalances can show up at any age. And struggling with them at various points throughout life is more common than most people realize.
Often, menstrual symptoms we are told are “normal” for women simply aren’t. They’ve just become common.
Before we get into what estrogen dominance actually is, we want to share something that may feel familiar. Beth’s story, and what she eventually learned.
It’s important you know that this blog post is for informational and educational purposes. It’s not meant to treat any health condition or to be prescriptive for anyone. If you have any medical condition, it is critical you work under the care and guidance of a licensed medical healthcare provider.
Estrogen Dominance: Beth’s Story
While Beth’s story is fairly severe, the underlying patterns and symptoms are things we see often. And chances are, parts of it will sound familiar to you, too.
“It started when I was a child.
Around 8 years old, I hit puberty before nearly all my friends. I was getting zits on my face and back and growing armpit hair. Soon I needed to wear a bra.
I started having periods just a couple of years later.
After just a few cycles, I started experiencing symptoms I was told were “normal.”
Symptoms during my period like:
- Cramps
- Clotting
- Heavy periods / heavy bleeding
- Low back pain
- Bloating
- Ravenous food cravings
- Anxiety
- Fatigue
I had all of those. And I also tended to get diarrhea, rashes, have trouble sleeping, and my skin would itch more than usual, too.
Those weren’t considered “normal” symptoms for periods, but each month, I got them along with everything else.
For me, the worst of these symptoms was what I initially thought were cramps.
They got progressively worse over the years. I had teeth-gritting cramping that would level me for 3 days every month. I would often miss a couple days of school because I just couldn’t function.
Eventually, even prescription pain meds didn’t take the edge off.
I remember one month the pain was so severe, I was doubled over and couldn’t walk. I couldn’t even form sentences. My parents thought my appendix must have burst.
After several hours in the ER, the doctors found that it wasn’t appendicitis after all. An ultrasound showed I had ovarian cysts that were rupturing. I was only 13 at the time.
After that episode, I was put on continuous birth control so that I would no longer menstruate. The doctors thought that if I didn’t have a period, I wouldn’t have pain.
No one was looking into estrogen dominance. And the contraceptive (birth control) I was put on … it was a synthetic estrogen. It added to my hormone imbalance and ended up making everything worse!
Much later I learned that ovarian cysts are associated with estrogen dominance.
I also learned that early puberty is associated with estrogen dominance.
That long list of “normal” symptoms? Also related to estrogen dominance.”
Our periods should be easy, not difficult. It’s just that estrogen dominance has become so common these symptoms are now sadly considered normal.
And the list of unusual symptoms Beth had like hives, itching, and insomnia? Those were mast cells and mediators (like histamine) triggered by estrogen dominance.
Let’s take a look at the connection between estrogen dominance and MCAS next.
MCAS and Estrogen Dominance: Understanding the Hormone and Mast Cell Connection
Not only is estrogen dominance responsible for some of the symptoms you’ve been told are “normal” for menstruation, but estrogen dominance also triggers your mast cells.
As you just read, it can be associated with symptoms that many people, even doctors, consider normal. Like:
- Cramps
- Clotting
- Heavy bleeding
- Irregular cycles
- Low back pain
- Bloating
- Fatigue
- Anxiety
- Headaches
- Brain fog
- And so much more!
Studies have shown that mast cells can be activated by hormones, particularly imbalanced estrogen.
Because mast cells are present throughout multiple systems (the skin, gut, respiratory tract, blood vessels, brain, and more) a hormonal trigger like estrogen dominance can show up as symptoms almost anywhere in the body.
Your mast cells actually have hormone receptors on them. This is how they can either be triggered or calmed down by the different hormones in your body.
If you have Mast Cell Activation Syndrome, estrogen dominance might be affecting you, too!
That’s what we want to look at today: hormones, estrogen dominance, and mast cells.
What Is Estrogen Dominance?
To understand estrogen dominance, you’ll first want a basic overview of hormones.
Estrogen and progesterone are the two main hormones to look at with estrogen dominance.
This is a copy of the DUTCH Complete Test for hormones. We’ll tell you more about what this all means in a minute. But we want to show you here because it’s a great visual of the different pathways of hormone production.
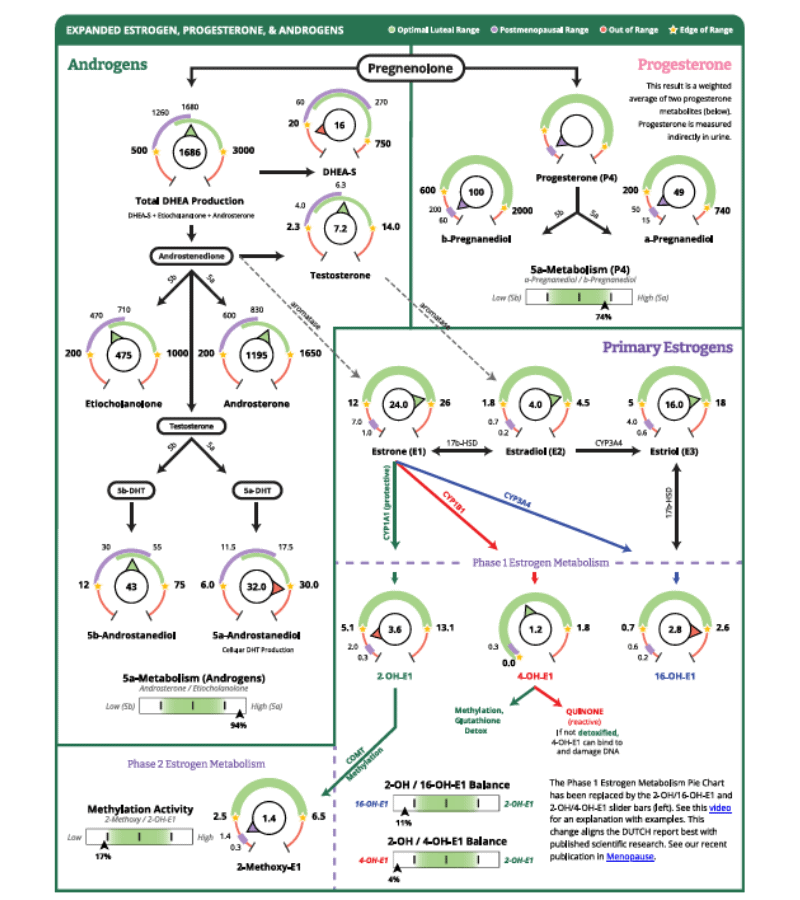
Your body’s hormone-producing glands use cholesterol to make what is called your steroidal hormones.
That’s why you need cholesterol. Cholesterol is converted into the master hormone, pregnenolone. You’ll see that at the top of the test result.
Then you’ll see that pregnenolone can become other hormones. Pregnenolone gets converted into:
- DHEA
- Estrogen compounds
- Progesterone compounds
- Cortisol
Related Post: Cortisol Imbalance and How to Support Your Adrenals with Mast Cell Activation Syndrome (MCAS)
Since we are talking about estrogen dominance, we’ll focus on estrogen and progesterone. Let’s take a closer look at the roles these two hormones play when they are balanced.
Estrogen and Progesterone
Estrogen is a female sex hormone.
Here’s what healthy levels of estrogen do for your body.
Estrogen has been shown to be important for:
- Puberty – promotes growth
- Pregnancy – supports full-term pregnancy and promotes development of the fetus
- Bone health – supports a protein important for bone cells
- Heart health – regulates cholesterol
- Sexual function – keeps the vagina lubricated
As you can see, estrogen plays several roles in maintaining good health.
Progesterone is the other hormone we want to consider with estrogen dominance.
Progesterone has been shown to be important for:
- Regulating the menstrual cycle
- Supporting pregnancy
- Metabolizing fat into energy
- Calming anxiety
- Preventing autoimmune diseases
- Promoting normal sleep patterns
- Restoring natural libido
- Calming mast cells
Again, all of these are important for good health!
Related Post: How to Balance Hormones Naturally with Mast Cell Activation Syndrome (MCAS)
So, that gives you a basic overview of what your hormones do when they are balanced. Next let’s look at what happens when they aren’t.
Estrogen Dominance: Imbalanced Hormones
Put simply, estrogen dominance is an imbalanced state of hormones where you have more estrogen than you should to be balanced.
Estrogen dominance isn’t always the same as high estrogen levels. That’s really important to know. You can have estrogen dominance even if your estrogen levels are normal.
Even in perimenopause or post-menopause, when women often have low hormone levels, you can still have estrogen dominance.
Estrogen dominance has been shown to be linked to:
- Acne
- Constipation
- Loss of sex drive
- Depression
- Weight gain
- Menstrual problems
- PMS (Premenstrual Syndrome)
- PMDD (Premenstrual Dysphoric Disorder)
- Increased risk of uterine and breast cancer
- Increased risk of cardiovascular disease
- Fibroids
- PCOS (Polycystic Ovarian Syndrome)
- Endometriosis
- Mast cell activation
Look at that last point again. That’s right. Estrogen dominance can trigger mast cells.
Then, you may also experience mast cell related symptoms like:
- Trouble sleeping
- Increased sensitivity to foods
- Constipation or diarrhea
- Pain
- Swelling
- Water retention
- Headaches
We’ll get back to how estrogen dominance and Mast Cell Activation Syndrom relate a little later.
Next, though, let’s look more at the main types of estrogen and the main types of estrogen dominance.
First, you’ll want to know about the 3 main types of estrogen.
This will make understanding the types of estrogen dominance a lot easier.
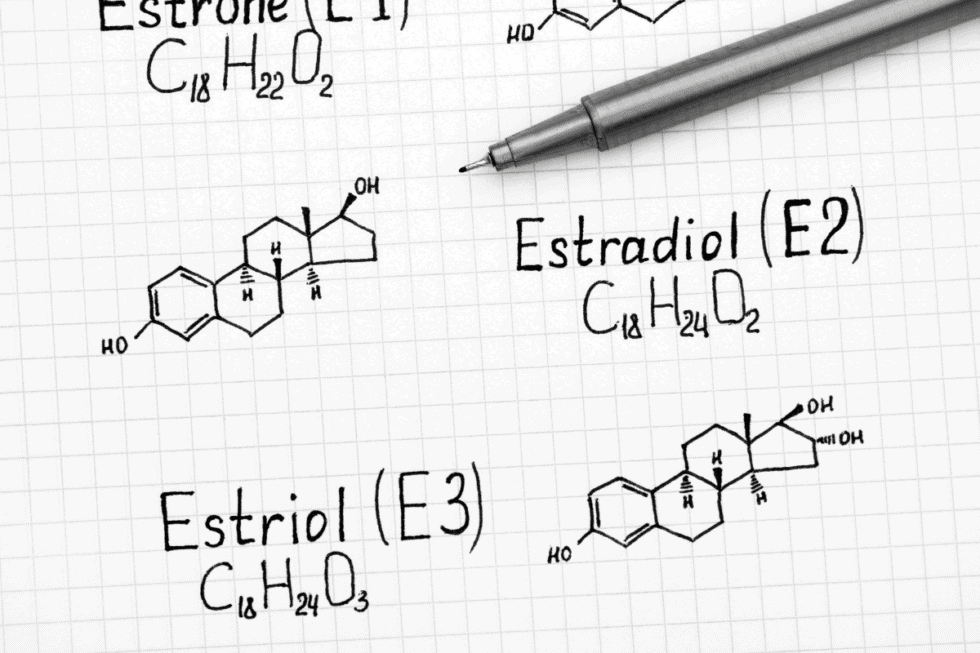
The 3 Main Types of Estrogen
E1 (estrone) is considered the “weaker” estrogen. E1 is usually the dominant form of estrogen during menopause. E1 is made in your liver and in your fat cells.
E2 (estradiol) is the strongest type of estrogen, made in your ovaries. It’s about 1000 times stronger than E3.
It’s important for bone health, mucous membrane lubrication, and energy. It plays important roles in the reproductive system, including menstruation.
Estradiol is sometimes referred to as “dirty” estrogen. This is because it can contribute to estrogen dominance and the problems associated with it.
It stimulates growth. Too much has been linked to breast, ovarian, and uterine cancers.
E3 (estriol) is a “protective” form of estrogen in your body. It’s made in your liver and breasts. You have high levels of E3 during pregnancy, but otherwise E3 levels are usually lower in the body.
You’ve been reading that estrogen dominance happens when hormones get out of balance.
Now, let’s take a look at the 3 main types of imbalances that lead to estrogen dominance.
3 Main Types of Estrogen Dominance
You can experience estrogen dominance from:
- More E2 estrogen than progesterone
- Estrogen metabolites out of balance
- Estrogen being broken down into damaging molecules
What does that mean? Here’s a breakdown.
1. More E2 Estrogen than Progesterone
The first one is fairly straightforward.
It just means your E2 estrogen levels are higher than your progesterone levels. Why is this a problem?
Take a look at the list below of how estrogen acts in estrogen dominance.
Estrogen Dominance can contribute to:
- Autoimmune disease
- Weight gain
- Migraines
- Depression/anxiety
- Insomnia and other sleep issues
- Decreased sex drive
- Triggers mast cells
Now, remember, we talked about estrogen also does good things for you. It’s just when there is too much estrogen that these negatives show up.
That’s because in a balanced state, these properties are usually counteracted by the properties of progesterone.
Think of it like a scale. With estrogen dominance, estrogen is weighing one side of the scale down. On the other side of the scale, there isn’t enough progesterone to balance.
From the list above, let’s take migraines as an example.
This isn’t saying that estrogen = migraines.
It’s saying that more estrogen than progesterone = migraines.
See, in a balanced state, the properties of progesterone help to prevent estrogen dominant symptoms, like migraines. The scale is balanced.
Here are some other roles of progesterone.
Progesterone can:
- Prevent autoimmune disease
- Help turn fat into energy
- Prevent migraines
- Act as a natural anti-depressant
- Promote normal sleep patterns
- Restore libido
- Stabilize mast cells
So, you can see that when the scale is tipped in estrogen dominance, all the good that progesterone does just isn’t enough to create a balance. Estrogen “weighs” too much.
In other words, when estrogen is dominant, it is more than the progesterone can counterbalance.
That’s one way you can have estrogen dominance that can contribute to Mast Cell Activation Syndrome or Histamine Intolerance.
Another way is when the different estrogens are out of balance.
2. Estrogen Metabolites Are Out of Balance
This type of estrogen dominance looks at your E1 and E2 levels in comparison with your E3 levels.
This isn’t a straightforward case of more E1+E2 than E3 = estrogen dominance.
It’s a bit more complex than that.
You may have run across the term “estrogen quotient.” That’s what’s used to look at the relationship between these three estrogens.
Estrogen quotient is a way of comparing the ratios of “dirty” estrogens to the protective ones. Remember that E3 is protective.
The estrogen quotient is determined by this formula:
Estrogen Quotient (EQ) = E3/(E1+E2)
The ideal estrogen quotient is 1.5 or higher. Using the DUTCH Complete Test from above, let’s see how to use this formula.
You’ll see that at the time of the test:
- E1 was 15
- E2 was 3.14
- E3 was 7.5
So, using the formula above, we first add E1+E2:
3.14 + 15 = 18.14. That is this person’s value for E1 plus E2.
Next, divide your E3 value of 7.5 by 18.14 (the sum of E1 + E2 from above).
This results in an estrogen quotient of .41.
Generally speaking, the higher your estrogen quotient, the better. But the example test above is well below the optimal of 1.5 or higher!
This low estrogen quotient is another form of estrogen dominance. You can see why testing all 3 types of estrogen is important.
Next, let’s look at one more form of estrogen dominance.
3. The Breakdown of Estrogen into Damaging Molecules
Estrogen dominance can also be the result of how the body is breaking down estrogen.
Your liver is responsible for breaking down estrogens. This is part of the process of eliminating estrogen from your body.
Estrogen can be broken down into these molecules (called metabolites):
- 2-hydroxyesterone (2-OH)
- 4-hydroxyesterone (4-OH)
- 16-alpha-hydroxyesterone (16-OH)
2-OH is a more protective metabolite. It works to block stronger estrogens that promote possible cancer growth.
4-OH can convert into something called quinones. These have been shown to damage DNA. It is thought to promote cancer by damaging DNA. It’s also sometimes called a “dirty” estrogen.
16-OH has been associated with inflammation, excess levels of the bad Omega-6 fatty acids, obesity, and hypothyroidism. It’s also been associated with an increased risk of breast cancer. For this reason, it’s also called a “dirty estrogen.”
If your liver is not able to break down the estrogens to eliminate them properly, it will generate too many “dirty” estrogens.
You can end up with more 4-OH or 16-OH if your liver needs support.
What you really want is more 2-OH than 4-OH and 16-OH.
This imbalance of estrogen metabolites is another way to experience estrogen dominance.
So, you’ve seen how estrogen dominance can really bring about some unwanted symptoms and conditions even if you don’t have Mast Cell Activation Syndrome.
But if you do have Mast Cell Activation Syndrome, estrogen dominance can be contributing to those symptoms, too.
Remember you read earlier that you can experience symptoms like hives, itching, and insomnia when ovulating. It turns out, these are mast cell symptoms. And they can be triggered by estrogen dominance.
Let’s look more at the connection between hormones and mast cells next.
Mast Cells, Progesterone, Estrogen and Histamine
Your mast cells are part of your immune system. And your immune and hormone systems are deeply interconnected. That means your hormones can directly affect your mast cells.
In fact, mast cells have receptors on them for both progesterone and estrogen. So, when those hormones are out of balance, your mast cells respond in kind.
When your immune response is already on high alert, hormonal imbalances can become a significant additional trigger, causing your mast cells to release mediators like histamine.
And estrogen imbalances don’t just trigger histamine release.
Beyond histamine, activated mast cells also release other inflammatory mediators like prostaglandins, heparin, and tryptase. Elevated prostaglandins are one reason period pain can be so severe in estrogen dominance. They trigger uterine contractions and amplify pain signaling.
Here’s where it becomes a loop. Estrogen stimulates mast cells to release more histamine. Rising histamine levels then drive more estrogen production. And on and on it goes.
So, estrogen dominance may be contributing to your symptoms AND to both mast cell activation and symptoms of Histamine Intolerance at the same time.
Let’s take a closer look at another way estrogen and histamine interact.
Estrogen and Histamine Intolerance
Here’s another way estrogen may be contributing to your Histamine Intolerance.
Excess estrogen can reduce an important histamine degrading enzyme called diamine oxidase (DAO). This DAO enzyme is produced naturally in your body to break down histamine.
If your body doesn’t produce enough DAO to keep up with your histamine load, that can lead to Histamine Intolerance.
You can get relief from symptoms of excess histamine with supports like:
- Taking out high histamine foods (fermented foods, avocado, spinach, chocolate, etc)
- Trying a low histamine diet
- Working toward better gut health, supporting SIBO
- DAO, quercetin, and antihistamines
- And working on balancing your hormones
But remember that with estrogen dominance, it’s not just about having elevated levels of estrogen. It’s about having an imbalance of hormones.
Low Progesterone and Mast Cell Stability: Why the Balance Matters
You read about the kind of estrogen dominance that occurs when estrogen levels are higher than progesterone levels.
When balanced, though, progesterone counterweights estrogen when it comes to mast cells and the release of histamine.
Progesterone can help stabilize mast cells AND progesterone helps stop mast cells from making more histamine.
This is because progesterone sends a signal through the mast cell hormone receptors to calm down.
This is a big reason the balance between estrogen and progesterone is so important. Supporting your progesterone will likely help with your histamine levels.
Keep in mind that we are talking about natural or bioidentical progesterone here. Synthetic progesterone medication often used for hormone replacement therapy (hrt) doesn’t usually have the same mast-cell calming effect.
Now, we get a lot of questions from women asking why they tend to get an increase in mast cell reactions during certain times of their menstrual cycle.
Some of these problems tend to happen around the time of ovulation (when the ovaries release the egg). That happens to be when estrogen levels peak.
This could be putting you in a more estrogen dominant state. And this estrogen dominance could trigger mast cells causing an increase in reactions.
Estrogen tends to be more dominant a couple days before your period starts, too. This is another common time women will have mast cell flares.
Does this make sense now as to why your mast cell symptoms can flare when your estrogen is out of balance?
Now, if any of this sounds like it might relate to you, we want you to know something really important. Testing is crucial. It’s not enough to go by symptoms alone.
Keep reading to learn why testing for estrogen dominance is so important.
Prefer videos? Watch the Live with our MC360 Clinic Team below:
Testing for Estrogen Dominance
It’s always important to test and not guess.
In Mast Cell Activation Syndrome all kinds of things can be happening. And some of your symptoms and conditions may not always be what they seem.
For example, we’ve worked with a few women who had classic estrogen dominance symptoms. But their tests showed they actually had low estrogen and high progesterone. So, something else was going on there.
So, you see how important it is to find good tests! Plus, if you know what kind of estrogen dominance you’re dealing with, you can target what to do about it better.
If the women above had just gone forward based on symptoms, usual protocols wouldn’t have worked. It may have even made them feel worse.
So, you’ll want to test first and check these different pathways.
Standard Hormone Tests
Now, with steroidal hormone testing, you’ll find several options.
There are saliva tests, blood tests, and urine tests that can test hormone levels.
It helps to know the pros and cons of testing methods to decide how to test. Different testing methods can have certain limitations.
Many people look at blood levels of hormones, which a lot of practitioners use.
Blood testing doesn’t account for how your hormone levels change throughout the day, though. And you rarely get the levels for E1, E3, and the various metabolites
And blood testing isn’t always accurate for cortisol. Especially if you’re feeling stressed when you get the blood draw. This stress can spike the cortisol in your blood and make it look higher than it usually is, or make low levels look normal.
You can also test for hormones with a saliva test. It can work well for estrogen, progesterone, DHEA, and testosterone. But the saliva test may not give the best results for your cortisol status.
As you can see, there are many options and pros and cons. Each practitioner has their preferences.
Our Favorite Test for Finding the Root Cause of Estrogen Dominance
We really like the DUTCH Complete Test. It’s a different type of urine test that is comprehensive.
The DUTCH test checks four or five dried urine samples over a 24-hour period.
What is a dry urine test? Instead of collecting liquid in a container, with a dry urine test you saturate a filter card with your urine sample. These samples are stable for several weeks and easy to ship.
The DUTCH report looks at the following:
- Estrogens: E1, E2, E3
- Estrogen metabolites:
- DHEA-S
- Testosterone (through metabolites)
- Progesterone (also through metabolites)
- Cortisone (storage form of cortisol)
- Cortisol
- Melatonin levels
- 8-OHdG (looks at DNA damage from quinones)
The hormones we’re talking about are more stable in urine. This means you can get a picture of what your hormone levels are like day to day.
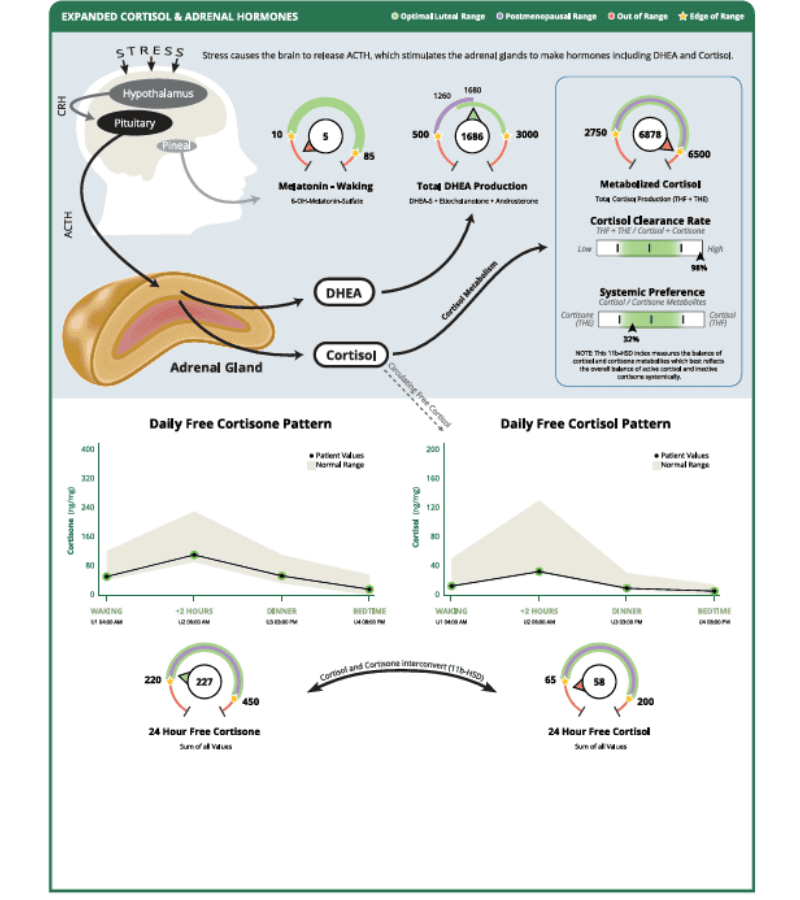
You also get a 4-point cortisol measurement. This means you can see your cortisol (and cortisone) patterns throughout the day. Here’s a look at the cortisol measurements from the same test.
We like to look at progesterone, estrogen, DHEA, testosterone, and cortisol together in the clinic. This is because these hormones are all created in your body from your master hormone, pregnenolone.
So, if you look at them together, you may see where problems with conversion are happening.
We like the DUTCH reporting because you can see the different pathways we talked about, too.
You can see in the report above that this person’s E2+E1 estrogens were higher than E3. They were also higher than their progesterone. All of that is valuable information in addressing what’s behind the imbalances.
Why We Prefer the DUTCH Complete Test for Estrogen Dominance and MCAS
This test result shows all 3 types of estrogen dominance we talked about before.
This is why it’s important to do testing. It really lets you know what you’re dealing with.
This can be especially important when you consider how to support yourself in balancing your hormones. If you really want to know what your estrogen balance is, the DUTCH Complete Test can help.
So, how can you order your own DUTCH test?
>>> You can get a DUTCH Complete Test for hormones on your own here without a doctor
Come back to this again once you get your own results!
Or a functional medicine clinician or functional practitioner who understands hormone health can help you interpret these results and build a plan that addresses the root cause, not just the symptoms.
Want to order the test but live outside the USA or Canada?
>>> You can order your own International DUTCH Complete Test for hormones here
What kind of mast cell flares related to estrogen dominance have you experienced?
More About Mast Cells and Hormones
- How to Reverse Estrogen Dominance Naturally: Information for Those with Mast Cell Activation Syndrome and Histamine Intolerance
- Cortisol Imbalance and How to Support Your Adrenals with MCAS
- BeSerene Review: Nervines and Adaptogens for Building Resiliency
- Nervous System Balance is Essential in Mast Cell Activation Syndrome and Histamine Intolerance
Some links in this website are affiliate links, which means Mast Cell 360 may make a very small commission if you purchase through the link. It never costs you any more to purchase through the links, and we try to find the best deals we can. We only recommend products that we love and use personally or use in the Mast Cell 360 practice. Any commissions help support the newsletter, website, and ongoing research so Mast Cell 360 can continue to offer you free tips, recipes, and info. Thank you for your support!
References
Bae, Y., Lee, S., & Kim, S. H. (2011). Chrysin suppresses mast cell-mediated allergic inflammation: involvement of calcium, caspase-1 and nuclear factor-κB. Toxicology and applied pharmacology, 254(1), 56–64. https://doi.org/10.1016/j.taap.2011.04.008
Binda, M. M., Donnez, J., & Dolmans, M. M. (2017). Targeting mast cells: a new way to treat endometriosis. Expert opinion on therapeutic targets, 21(1), 67–75. https://doi.org/10.1080/14728222.2017.1260548
Bonds, R. S., & Midoro-Horiuti, T. (2013). Estrogen effects in allergy and asthma. Current opinion in allergy and clinical immunology, 13(1), 92–99. https://doi.org/10.1097/ACI.0b013e32835a6dd6
Boyce, J. A. (2007). Mast cells and eicosanoid mediators: A system of reciprocal paracrine and autocrine regulation. Immunological Reviews, 217(1), 168–185. https://doi.org/10.1111/j.1600-065X.2007.00512.x (Supports prostaglandins released by mast cells)
Christy, A. L. (2007, September 1). The Multitasking Mast Cell: Positive and Negative Roles in the Progression of Autoimmunity. The Journal of Immunology. https://journals.aai.org/jimmunol/article/179/5/2673/81297/
Cleveland Clinic. (2022, January 5). Estrogen: What It Does and 5 Benefits. Retrieved February 2, 2022, from https://health.clevelandclinic.org/what-does-estrogen-do/
Cleveland Clinic. (n.d.). Endometrial Hyperplasia: Causes, Symptoms & Treatment. Retrieved February 2, 2022, from https://my.clevelandclinic.org/health/diseases/16569-atypical-endometrial-hyperplasia
Ferlemi, A. V., & Lamari, F. N. (2016). Berry Leaves: An Alternative Source of Bioactive Natural Products of Nutritional and Medicinal Value. Antioxidants (Basel, Switzerland), 5(2), 17. https://doi.org/10.3390/antiox5020017
Jonassen, J. A., & Rao, C. V. (2021). Luteal phase defects and progesterone insufficiency. Seminars in Reproductive Medicine, 39(3–4), 143–152. (Supports luteal phase / low progesterone context)
Jensen, F., Woudwyk, M., Teles, A., Woidacki, K., Taran, F., Costa, S., Malfertheiner, S. F., & Zenclussen, A. C. (2010). Estradiol and progesterone regulate the migration of mast cells from the periphery to the uterus and induce their maturation and degranulation. PLOS ONE, 5(12), e14409. https://doi.org/10.1371/journal.pone.0014409 (Directly supports luteal phase, low progesterone, and mast cell stability arguments)
Kim, M., Lim, H. S., Lee, H. H., & Kim, T. H. (2017). Role Identification of Passiflora Incarnata Linnaeus: A Mini Review. Journal of menopausal medicine, 23(3), 156–159. https://doi.org/10.6118/jmm.2017.23.3.156
Kolan, A. (2014). VA.gov | Veterans Affairs. US Department of Veterans Affairs. Retrieved February 7, 2022, from https://www.va.gov/WHOLEHEALTHLIBRARY/tools/estrogen-dominance.asp
Malekinejad, H., & Rezabakhsh, A. (2015). Hormones in Dairy Foods and Their Impact on Public Health – A Narrative Review Article. Iranian journal of public health, 44(6), 742–758.
Marhol, A., MD PhD. (2022, January 7). What Happens to Hormone Levels During the Menstrual Cycle? Flo.Health – #1 Mobile Product for Women’s Health. Retrieved January 30, 2022, from https://flo.health/menstrual-cycle/health/period/hormone-levels-during-cycle
Miao, S., Yang, F., Wang, Y., Shao, C., Zava, D. T., Ding, Q., & Shi, Y. E. (2019). 4-Hydroxy estrogen metabolite, causing genomic instability by attenuating the function of spindle-assembly checkpoint, can serve as a biomarker for breast cancer. American journal of translational research, 11(8), 4992–5007.
Pajewska, M., Łojko, M., Cendrowski, K., Sawicki, W., Kowalkowski, T., Buszewski, B., & Gadzała-Kopciuch, R. (2018). The determination of zearalenone and its major metabolites in endometrial cancer tissues. Analytical and bioanalytical chemistry, 410(5), 1571–1582. https://doi.org/10.1007/s00216-017-0807-7
Samavat, H., & Kurzer, M. S. (2015, January 28). Estrogen metabolism and breast cancer. ScienceDirect. Retrieved January 30, 2022, from https://www.sciencedirect.com/science/article/abs/pii/S0304383514002365
Schütz, K., Carle, R., & Schieber, A. (2006, October 11). Taraxacum – A review on its phytochemical and pharmacological profile. ScienceDirect. Retrieved January 31, 2022, from https://www.sciencedirect.com/science/article/abs/pii/S0378874106003576?via%3Dihub
University Of Maryland, Baltimore. (1998, March 14). Lack Of Estrogen Causes Miscarriage: Restoring Normal Estrogen Levels Maintains Pregnancy. ScienceDaily. Retrieved January 31, 2022 from www.sciencedaily.com/releases/1998/03/980314120120.htm
University of Rochester Medical Center. (n.d.). Chaste Tree – Health Encyclopedia – University of Rochester Medical Center. Retrieved January 31, 2022, from https://www.urmc.rochester.edu/encyclopedia/content.aspx?contenttypeid=19&contentid=ChasteTree
Wszelaki, M. (2020, June 13). Are Histamines Wrecking Your Hormones? HormonesBalance.Com. Retrieved January 30, 2022, from https://hormonesbalance.com/articles/are-histamines-wrecking-your-hormones/
Wszelaki, M. (2021a). Overcoming Estrogen Dominance (1st ed.). self-published.
Wszelaki, M. (2021, March 10). How to Use Herbs for Estrogen Dominance. HormonesBalance.Com. https://hormonesbalance.com/articles/7-herbs-manage-estrogen-dominance-pms-breast-lumps-cellulite/
Wszelaki, M. (2021, May 20). Best Supplements for Estrogen Dominance. HormonesBalance.Com. https://hormonesbalance.com/articles/best-supplements-for-estrogen-dominance/
Wszelaki, M. (2021, September 30). More Than Just A Weed: How to Use Dandelion For Detox and Hormones. HormonesBalance.Com. Retrieved February 2, 2022, from https://hormonesbalance.com/articles/more-than-just-a-weed-how-to-use-dandelion-for-detox-and-hormones/
Zierau, O., Zenclussen, A. C., & Jensen, F. (2012). Role of female sex hormones, estradiol and progesterone, in mast cell behavior. Frontiers in immunology, 3, 169. https://doi.org/10.3389/fimmu.2012.00169



Thank you so much for sharing the knowledge.. So is it possible or common that you react to even low histamine foods around the time of ovulation when you have mast cell activation symdrome? I am in ovulation now and reacted to my staple vegetable yesterday. Looking back to my journals I found it is not always but I had it before,too around the time of it.
I was very sick for months not knowing I had mold toxicity, my period stopped for three months. since I reduced mold exposure I’ve been feeling better and last month my period returned, however I’ve been getting relapses and I don’t know why, do you think estrogen may have something to do with it?
btw I found this article very intriguing, thank you so much for this article
It’s great that your cycle returned with reduced mold exposure. It might be worth paying attention to when in your cycle these relapses are occurring and if there’s any pattern there. Since we are unfamiliar with your individual case we cannot say for certain if what you are experiencing is estrogen related, we highly suggest bringing up these issues/concerns with your licensed medical provider.
I have had MCAS since childhood and recently have been experiencing bad anxiety/depression, headaches and trouble sleeping on a cycle of every 2 weeks for the past 5 months. I am convinced hormones are in play. Can you let me know what the ideal treatment would be? I am going to see a new doctor next week, but most doctors are unfamiliar with MCAS. I’ve heard the treatment protocol is to supplement with progesterone. Can you advise?
Hi Sarah. We’re sorry to hear you’ve experienced MCAS since childhood and are recently having trouble sleeping. Headaches around hormonal changes are not uncommon, but without knowing your individual case, it is hard to say what might be going on for you. You may find Beth’s recent FBL with Dr. Tania Dempsey on hormones to be helpful in coming up with an idea where to start first. You can find that replay here: https://www.youtube.com/live/DQEHG1zvcJE?si=TV23V6xUdtDi8cVU
Your article has been most informative and answers many questions to the symptoms I have been experiencing for years. I am post-menopausal for 5-6 years now but recently started having serious symptoms. My GYN diagnosed estrogen dominance based on symptomology and refuses to do any testing to confirm my hormone levels. I also have MCAS and take a daily H1 blocker (about 7 years). I have been taking progesterone for three weeks now and feel worse each week that goes by! I believe your article explains what’s happening – my estrogen dominance is feeding my MCAS in a vicious cycle that is resulting in very bad symptoms. My docs are not sure how to address this but keep increasing my progesterone dosage in the hopes of finding a balance. I think I will spring for the Dutch Test as this looks very comprehensive and could give me a greater understanding of my ACTUAL problem. Thank you for sharing your journey!
Thank you so much for this helpful article. You mention that synthetic progesterone does not have the same regulating effects, so I’m wondering how we can support endogenous hormone balance? Supporting the liver feels important, but what else would you recommend (perhaps you have another article you could link)? Thanks!
Hi Lizzy, you can learn more about naturally balancing estrogen in this blog: https://mastcell360.com/reverse-estrogen-dominance-naturally/
Ah, this explains my life! Thanks for this great info. My estradiol was 455 a few years ago, which my doc said was the highest she’d ever seen. I know I had estrogen dominance probably by the time I was 12. I was gaining weight in ways that made no sense. I had one natural period when I was 14 and never had another. I was on bcp from age 16 until I had my uterus removed when I was 30. Then when I went off bcp after the surgery it was about a year and a half later that my ovaries had exploded with hemmorhagic cysts. I was supposed to have my ovaries removed 3 days after they found it, but the main cyst they were worried about ruptured beforehand, so then they said I didn’t have to have the surgery. So then I had another 22 massive cyst ruptures over the next 10 years. And then I ended up with MCAS. Yaay! I have made a lot of progress w/the MCAS over the last year but it’s still a journey. I don’t get obliterating migraines anymore but I’ll get inexplicable fatigue and other weird symptoms. Btw, the most effective treatment for my cysts was an infrared light panel, and the most effective treatment for MCAS has been hydrogen. It’s the one thing that acts as a major anti-inflammatory, anti-oxidant and supports ATP production that doesn’t cause a flare-up. Everything else I tried that does any of those things caused me to have a bad reaction. Now I can tolerate a little more glutathione, etc., etc.
Hi Ava! We are so glad to hear that you’ve found somethings that works for you! Wishing you all the best on your continued healing.
Thank you for sharing, is it interesting for a man to test all these hormones and therefore to do the Dutch Test ? Thank you.
Hi Fred,
Thanks for reaching out with your question!
Yes, men can do a DUTCH test; the report will reflect appropriate levels for men rather than for women, as they will be different.
Best,
Zack